


EKGs pt 2 -- Heart Blocks
QRS waves and all the exciting things that can happen to them!

So here’s the link to pt one of my EKG overview for laymen, in which we covered the P wave on the EKG, which indicates atrial action.
Now it’s time to talk about ventricles! (Remember, again, I’m not your cardiologist ;))
The ventricles are the real work horse/s of your heart, since they’re doing most of the true pumping action. Let’s look at our normal EKG again:

Okay, so, see the big pointy bit? (You’ve seen it before on TV shows, I know you have.) That’s the QRS, which is the reading of electricity moving through and causing contractions of the ventricles. (Makes sense that it’s a bigger wave than the P wave, huh? In that the ventricles are bigger?)
So what a normal QRS is telling us is that your heart is firing normally, in the exact right sequence to prime your ventricles with blood (via atrial squeeze, that P-wave) and then to shoot the blood out to your lungs/body with ventricle action.
Now that we know what normal looks like, how come sometimes things get screwed up (and how can we see that on an EKG?)
Let’s go back to the diagram of the heart’s electrical anatomy — remember the SA (sino atrial) node was all about the atria, and it also shoots a message to pump to the AV (atrioventricular node) — which, and we didn’t talk about this last week — shoots a message down through the center of your ventricles to tell them to pump, via the bundle branches, as show below:

(AS AN ASIDE: You might have heard of bundle-branch blocks before — they occur when there’s been damage of the cardiac tissue the nerves conduct through, and they’ll mess up that nice sharp inverted V of a normal QRS, depending on the view from the 12 lead. I wanted to acknowledge them, but they’re beyond the scope of this newsletter.)
Our last component — before we start doing additive things and it gets fun, bear with me! — is the T-wave.
Let’s look at normal one more time (this’ll help for compare and contrast later, too, swear!):
The T wave represents the repolarization of your ventricles. It’s like a little rest stop, if you’re familiar with musical annotation — it shows that your ventricles are getting reset, so that they can do it all again.
Okay — now that we know that the P-wave = atria, the QRS = ventricles, and the T-wave = ventricular reboot, let’s go macro before we get micro :D
I apologize that this image is blurry, but it was the best combo image, and I had to size it up:
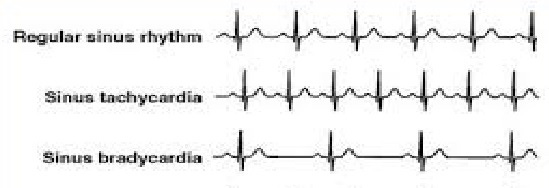
(The word ‘sinus’ in all these cases indicates that the sinoatrial (SA) node is in charge of creating the electrical impulses.)
Normal sinus rhythm: P-wave, QRS-wave, T-wave, all is well in the world. Heart’s truckin’! Toot-toot!
Sinus tachycardia: your heart rhythm is normal (which mean’s the muscle’s fine), just fast — but we haven’t lost any waves. You can still see the P wave and the T wave just fine. Your heart just decided to kick it up a notch — maybe you were hiking and saw a bear. (Or your ex. Who might also be a bear.)
Sinus bradycardia: again, all waves are present, it’s just everything’s movinnnnnggg slooowwwww (which is because the SA node is firing slowly. It’s not necessarily indicative of muscular damage to the heart…yet.)
Problems start to come in though when:
1) Your heart goes too fast
2) Your heart goes too slow
3) Electrical conduction issues in your heart mean that the waves start to disassociate from one another — these are called heart blocks.
D) ALL OF THE ABOVE. Sometimes in rapid sequence, aie!
(We’re gonna cover heart blocks first, because too fast and too slow are more advanced/emergency concerns, and they’ll be part three, early next week :D.)
So now that we know what a normal rhythm looks like, we can appreciate when things are ‘off’.
(And you’re going to laugh, but there’s not an ACLS certified nurse on the planet who doesn’t know this stupid poem.)

First degree heart blocks indicate a lag between that SA node P-wave-causing atrial-firing, and the QRS getting the ‘squeeze!’ memo. This could be caused by electrolyte issues, medication, heart damage, etc. You likely won’t have any symptoms, but if it’s treatable you should.
Now, remember how normal rhythms should have P-QRS-T?

(Did I try to make that look like a dick and balls, so it’d be memorable? Kinda! But I only have a touch pad, dammit ;P.)
This is called a second degree type 1 AV block or a Wenkebach (the guy who found it, and useful for when you need your poem to rhyme.)
It represents conduction issues with your AV node, you know how you can tell?
Because your P waves are all still there. Your SA node is just P-waving along, but for some reason your AV node isn’t getting the message to fire. It’s all, “wait for my QRS…wait for it…waiiiiittt for itttttt…whoops, I forgot one!”
So you can see above that:
1) The P to QRS interval is getting longer with each successive beat and
2) Eventually it skips a QRS entirely! There’s two Ps, but no QRS between them!
This is a pretty benign rhythm, but you might feel dizzy (your ventricles are skipping blood-pushing QRS beats periodically after all) and if your MD can figure out what’s causing it and fix it for you, you should.
Now we’re getting into the baddies, starting with a Mobitz II (aka second degree AV block type 2)

In this strip, the P to QRS ratio stays the same…it’s just sometimes there aren’t any QRS at all.
We’ve gone from a ‘sometimes I don’t get the memo to beat’ situation to ‘memo, what memo? who said anything about a memo?’
This rhythm is bad mostly because it can indicate the beginnings of disassociation between the SA node and the AV node entirely.
Which leads us to the very deadly type 3 heart block…

You don’t have to be a cardiologist to know that this rhythm sucks.
What it’s showing is your SA node giving you P-waves when it feels like it, and your AV node giving you QRSs when it feels like it — but there’s no coordination between the two nodes to give you an organized, functional rhythm.
This image is a little more subtle but will still get the point across:

There’s P waves, doot-doot-doot’ing along, but they bear no relationship to the QRSs that are also there, doing their own thing. Which is why sometimes they’re near, sometimes they’re far — does anyone have a coordinated plan for this heart to beat or that blood to flow? Nope!
Here’s another, where someone helpfully annotated the atrial p-wave and the ventrical’s QRS attempts:

The owner of this heart probably feels like they’re gonna die — because they are, unless they get help.
More about how to stop that in part 3, next week!
— Cassie